Christmas Blues
CHRISTMAS BLUES
I was meant to spend my day diving on Christmas Day. I had it all planned out down to the tiniest detail.
I’d wake up at 6 AM, pick up Klaus and Yanika fron the dive shop and get all our gear set up. Then we’d drive to the ferry terminal, head over to Gozo and spend our day diving there. We’d be going to a famous shipwreck, then to a cave, and then wherever we felt like going. We’d come back late in the afternoon, have a drink and that’d be it – the perfect Christmas. That’s how I’d spent my last Christmas, after all. To be back in Utila with all my friends… I would’ve given anything. Instead, I had to settle for this plan. Until, that is, we realised we’d be facing two-metre-high waves. Had we stuck to our original plan, I guess we would’ve gone surfing rather than diving.
And so, I took an extra shift at ED. I don’t really celebrate Christmas anyway, so why the hell not? I’d be giving my friend a chance to hang out with her family and enjoy the festivities, while I’d earn a little extra money in the process. Also, admittedly, there was nowhere else I would have rather been. I don’t really fancy the idea of spending my day at home with my family.

Business as Usual
The atmosphere at ED was as jolly as it could possibly be. Most doctors were wearing Christmas sweaters, Santa hats and God knows what else. I, on the other hand, wore my basic blue scrubs. I’m not really a fan of having to tell someone their relative has died or doing CPR on someone with jingly bells over my head. Plus, I’m not a fan of Christmas anyway.
It’d be just like any other day. I mean, yeah, sure, I’d probably greet my patients with the “Merry Christmas” that was expected of me, though under the circumstances, it might easily be in bad taste. But apart from that? It’d be business as usual. People get injured and die on Christmas Day much like they do on any other day – hence the waiting room full of patients waiting to be seen. That, to me, was kind of a gift. It would distract me from the fact that I was meant to be a few dozen metres underwater. Instead, I’d be drowning in cases.
In fact, it was just like any other shift. A patient who came in with chest pain, whom I discharged after all his investigations came back normal. Another who had thrown a glass jug at his mother, whom I admitted to the psychiatric hospital. One who presented with an asthma attack, whom I admitted for further treatment. A guy with gastroenteritis who needed intravenous hydration. You know, the same old, same old. Business as usual.
Strike One
Then came that one patient. A young woman who had found out she was pregnant that same day. She came in ’cause, at one point, she felt weak, developed abdominal cramps, vomited and then passed out for a few seconds.
Probably some pregnancy jitters, we all assumed. In fact, the second I went into the room, I wanted nothing more than to get the case over and done with, just so I could see more patients. Only she barely spoke English and her partner seemed focused only on his version of the story, meaning I’d need to spend more time in that room than I’d otherwise have to. The history was convoluted and all over the place. Things just didn’t add up. I was sure they were exaggerating. Of course, I’d run all the necessary tests and bloods, just to exclude anything serious, but I was sure she was just being overly dramatic given her unexpected pregnancy. “It’s just stomach cramps!” insisted the triage nurse, and, given her vague symptoms, I was kinda sure of it myself.
As usual, I took some bloods. Given that she was pregnant, I wanted to avoid imaging with ionising radiation unless it became absolutely necessary, and at that point, blood tests and bedside assessment were the quickest tools available to me. The venous blood gas, a point-of-care test that you can obtain in a matter of seconds, was alarming to say the least. Something was seriously wrong. She was severely acidotic, with her blood lactate level through the roof. CRAP! Suddenly, it wasn’t just cramps or pregnancy jitters. Suddenly, it was something far more serious than that. A new pregnancy, abdominal pain, vomiting, collapse, acidosis…
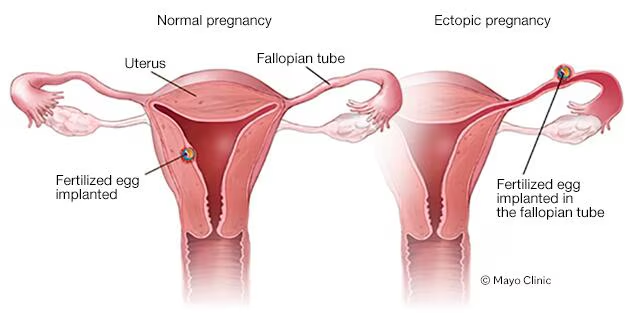
There was no other way around it. It was most probably a ruptured ectopic pregnancy – when a pregnancy implants outside the uterine cavity, most commonly in the fallopian tube, and then ruptures, causing internal bleeding.
Strike Two
This is where things get complicated. For some reason that I cannot possibly fathom, her blood pressure had not been recorded at triage.
Using the Emergency Severity Index scoring, blood pressure isn’t one of the vitals used to classify the patient’s urgency (which I think is quite idiotic, if I may so myself). So really and truly, I can[t quite blame the triage staff. Then, when I picked up the case, I asked for it to be measured. After I had seen her, I asked once again. Each time, the request seemed to disappear into the general chaos of the department. In hindsight, I should’ve just measured it myself. Thing is, I underestimated the situation and assumed it would get done eventually.
Well, I was wrong. After alerting my seniors, their first question was about her blood pressure – one I certainly couldn’t answer, given that no one had taken it yet. Strike number two. I stood there feeling like a blithering idiot, knowing very well that it should have been one of the very first things I had checked.
By the time we got around to it, she was already hypotensive – her blood pressure tanking. Her heart rate shot up, trying to compensate for the blood she was probably losing into her abdomen. A bedside ultrasound confirmed just that. I quickly explained to the patient and her partner what we were suspecting, then called the gynaecology team at once. They insisted the patient could be transferred to their department – something I flat-out rejected given how unstable she was.
We transferred her to the resuscitation room, and, just in the nick of time, the entire team was assembled.
The Hurricane
By that point, the patient was stuck in the middle of a hurricane of activity. We noted her to be cold and clammy, her pulse weak and thready.
On one side, there were the gynaecologists doing the ultrasound and trying to confirm the diagnosis. On the other, there was me trying to get a second venous access while the nurses hooked her up to oxygen, monitoring and God knows what else. I could only imagine what was going on in her head, with us speaking in English and Maltese – two languages she could not understand. I tried to reassure her along the way, my humanity and compassion finally kicking in. That morning, this completely healthy young woman had woken up to celebrate Christmas Day with her partner, found out she was pregnant, and now lay here on a trolley about to be transferred to theatre for life-saving surgery.
In the midst of it all, I was also worried about our performance. Had we checked her blood pressure from the very beginning, she might not have decompensated in the way she did. We could have sped up the process by at least half an hour and maybe prevented her from deteriorating, instead of having to do damage control so late in the process. Under such circumstances, every minute is precious. But forget all about the possible medicolegal repercussions. If she wouldn’t pull through, her partner would lose the love of his life and their baby in one fell swoop. Who the hell could ever convince me that their blood wasn’t on our hands if that were to happen?
Despite our collective shortcomings – which I felt mostly responsible for – somehow, luckily, everything went well. We managed to transfer her to theatre safely. What happened then… that was up to the gynaecology team. I just hoped everything would be fine.
The Lesson I Didn’t Ask For
This experience taught me a few things, to say the least. Ones that perhaps I already knew about – ones that tend to become less important when you’re lost in routine.
First of all, I’d no longer underestimate anyone’s presenting complaint, even if other colleagues insist it’s nothing to make a fuss about. Second, if I’d want something done urgently, I’d have to be ready to do it myself. While being able to delegate is part of what makes a doctor good at their job, I wouldn’t ever let delegation get in the way of patient care again. Third, if I had to stand up to other specialties when it comes to reviewing patients who need urgent input, then so be it. The patient could very well have died while waiting for the gynaecology team to see her.
Fourth? I have to sharpen my clinical acumen. While abdominal pain, vomiting and passing out can sometimes be explained by normal physiological processes in gastroenteritis or early pregnancy, the first thing that should have come to my mind was a ruptured ectopic pregnancy.
While we have excellent senior support at ED, I was now becoming more senior myself, and I would be expected to measure up to the level of excellence that entails – even in areas where I’d have less experience. I had to be better. I would be better.